Case study 3: Shawn
- Shawn’s parents took him to the clinic because he had acquired a waddling way of walking and was complaining of pain in his hips and calves
- During the consultation, his parents told the physician that in infancy Shawn had suffered from repeated vomiting and problems with sucking and chewing. Developmental delays in speech and cognition had subsequently been identified
- The physician conducted a physical examination and then referred Shawn for a hip X-ray and a neurologic consultation
Patient file
Table 1: Patient characteristics and observations from physical examination
| Age | 10 years |
| Tendon reflexes | Absent throughout. Sensation and strength preserved |
| Other observations | Bilateral pes cavus Trendelenburg gait Difficulty maintaining balance and poor ability to hop |
X-ray findings

- How do you interpret these findings?
- When examining these test results, would you consider a diagnosis of MPS?
Figure 1: Pelvis. Note acetabular dysplasia, coxa valga, and moderate to severe superolateral subluxation of both femoral heads, with findings more pronounced on the left. The acetabular angle is 58°, which is wide compared to the normal value of less than 42° for children aged 101
Interpretation
- Shawn’s hip dysplasia is characteristic of a number of diseases, including MPS, and various musculoskeletal-neurological disorders
- Acetabular dysplasia, coxa valga and subluxation of the femoral heads are commonly seen in patients with MPS2. However, although there is dysplasia on both sides, it is more pronounced on the left. This would be unusual in patients with MPS where symmetrical bilateral dysplasia is more generally seen
- The pes cavus and the reported oromotor difficulties in infancy are also not observed in patients with MPS
- These features are, however, associated with Charcot–Marie–Tooth (CMT) disease, one of the most common inherited neurologic disorders
- CMT is characterized by reduction in peripheral nerve conduction velocity due to abnormalities in nerve myelin. It leads to progressive weakness and muscle wasting, mainly in the feet and legs. The hands may also be affected1
Diagnosis
- The acquisition of a waddling gait and onset of hip and leg discomfort at 10 years of age, the bilateral pes cavus and the history of oromotor difficulties and developmental delays, led Shawn’s physician to suspect a neurologic disorder
- He referred Shawn for neurologic consultations. There was increased muscle tone in the ankles and absence of tendon reflexes. MR imaging revealed enlargement of the lumbar and sacral nerve roots (Figure 2)
- Subsequent genetic testing reported duplication of the gene for peripheral myelin protein, PMP22. This mutation causes CMT type 1A disease which is the most frequent form of CMT
- Because of variable clinical signs and symptoms with CMT 1A, diagnosis may be delayed. Hip dysplasia, particularly presenting in older children (> 8 years), may be one of the initial signs of the disease
- The origin of the dysplasia in CMT disease is thought to be neuromuscular deficits. These lead to progressive weakening of the proximal muscles which gives rise to changes in gait, such as pronounced external rotation at the hips and decreased hip adduction. Alterations in joint mechanics in the hip occur, resulting in subluxation and secondary acetabular dysplasia1
MRI findings
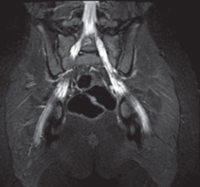
Figure 2: Pelvic MRI showing enlargement of lumbar and sacral nerve roots1.
Treatment and follow up
- Following diagnosis, Shawn was referred for hip surgery. He underwent triple innominate osteotomy and proximal femoral varus osteotomies
- As a result of the procedures, Shawn had greatly reduced pain in his left hip. However, he developed peroneal nerve palsy after surgery to the right hip. This is a common finding in patients with CMT
- Orthoses to be worn at night were recommended to correct Shawn’s foot drop1
- Bamford NS, et al. Dev Med Child Neurol 2009;51:408–411.
- Bamford NS, et al. Dev Med Child Neurol 2009;51:408–411.
- White KK and Harmatz P. J Ped Rehab Med 2010:47–56.